Endoscopic spine surgery for the treatment of lumbar disc herniation
Endoscopic spine surgery for the treatment of lumbar disc herniation
Information for patientsLumbar disc herniation is one of the most common causes of lower back pain and pain that travels down one leg, commonly known as sciatica. In many cases, this problem can improve with medical treatment, relative rest, physical therapy, and changes in physical activity. However, when the pain is intense, persistent, or accompanied by numbness, tingling, or weakness, it may be necessary to evaluate surgical treatment.
One of the modern options for treating lumbar disc herniation is endoscopic spine surgery, a minimally invasive technique that allows the surgeon to remove the fragment of disc that is compressing the nerve through a small incision and with less damage to the muscles of the back.
What is a lumbar disc herniation?
The lumbar spine is made up of bones called vertebrae. Between each vertebra is a structure called an intervertebral disc, which works as a natural shock absorber.
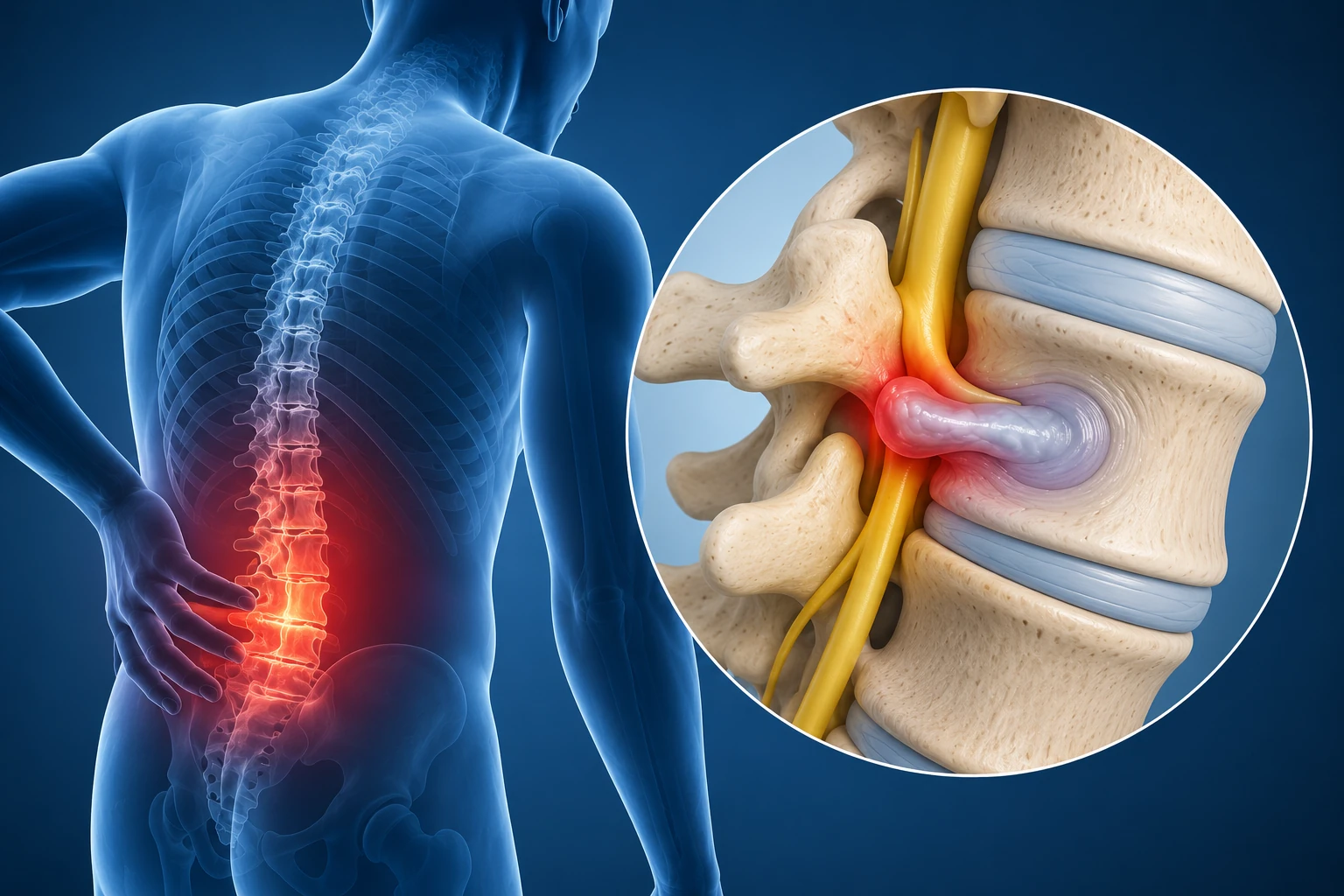
Each disc has a more resistant outer part and a softer inner part. When a portion of the disc moves out of place, it can compress or irritate a nerve. This is called a lumbar disc herniation.
When the nerve is compressed, the patient may experience pain that travels from the back to the buttock, thigh, leg, or foot. This pain may be accompanied by a burning sensation, cramping, tingling, numbness, or weakness.
Most common symptoms
Symptoms may vary depending on the affected nerve. The most common symptoms are:
- Lower back pain.
- Pain that travels down one leg.
- Tingling or numbness.
- Burning, electric shock-like, or cramping pain.
- Weakness when walking, climbing stairs, standing on tiptoes, or lifting the foot.
- Pain that worsens when sitting, bending over, lifting weight, coughing, or sneezing.
- Difficulty working, sleeping, walking, or performing normal activities.
Do all disc herniations require surgery?
No. Many disc herniations can improve without surgery. Initial treatment usually includes medications, physical therapy, specific exercises, reducing activities that worsen the pain, and, in some cases, injections to reduce inflammation around the nerve.
Surgery is mainly considered when:
- The pain does not improve with conservative treatment.
- The pain clearly travels down one leg.
- The MRI shows a herniation that matches the symptoms.
- There is muscle weakness.
- There is significant or progressive numbness.
- The pain significantly limits daily life.
- There are signs of severe nerve compression.
Surgery should not be indicated only because an MRI shows a herniation. Many people may have disc changes without having significant symptoms. The most important thing is that the symptoms, medical examination, and imaging studies match.
What is endoscopic lumbar surgery?
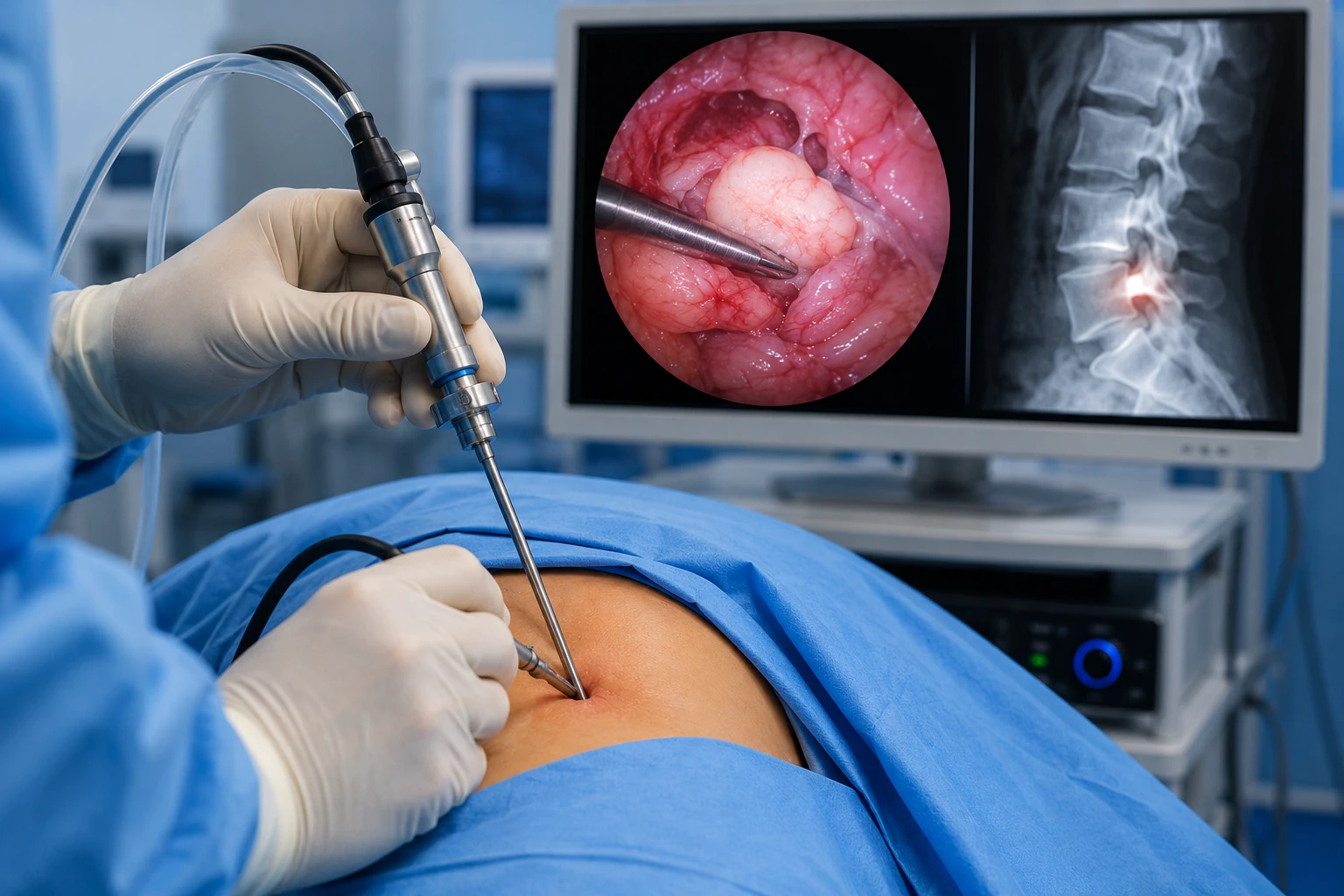
Endoscopic lumbar surgery is a minimally invasive technique that uses a thin camera, light, and special instruments to reach the disc herniation and remove the fragment that is compressing the nerve.
The surgeon watches the procedure on a screen, which allows precise work through a small incision. In many cases, this technique helps better preserve the muscles, ligaments, and bones of the spine.
The goal of surgery is not to remove the entire disc, but only the fragment that is causing pressure on the nerve.
How is the surgery performed?
In simple terms, the procedure is performed as follows:
- The patient is taken to the operating room.
- Anesthesia is administered, usually general anesthesia.
- The patient is positioned face down.
- The exact level of the herniation is located using X-rays during surgery.
- A small skin incision is made.
- An endoscopic system with a camera is inserted.
- The nerve structures and the herniated disc fragment are identified.
- The disc fragment compressing the nerve is carefully removed.
- The surgeon confirms that the nerve has been decompressed.
- The instruments are removed and the wound is closed.
In selected cases, surgery may involve a short hospital stay. Some patients may go home the same day or the following day, depending on their recovery and the medical instructions.
Potential benefits of endoscopic surgery
Endoscopic surgery may offer several benefits in carefully selected patients:
- Smaller incision.
- Less muscle damage.
- Less bleeding.
- Less pain after surgery.
- Faster recovery.
- Shorter hospital stay.
- Smaller scar.
- Faster return to everyday activities.
- Less manipulation of healthy structures.
- Good visualization of the area of nerve compression.
It is important to clarify that these benefits may vary from one patient to another. The result depends on the type of herniation, its location, the duration of symptoms, the presence of neurological damage, and the experience of the surgical team.
Who may be a candidate for endoscopic surgery?
A patient may be a candidate when they have:
- Lumbar disc herniation confirmed by MRI.
- Pain that travels down the leg and matches the compressed nerve.
- Persistent pain despite medical treatment and physical therapy.
- Weakness in the leg or foot.
- Numbness or sensory changes.
- Disabling pain that affects quality of life.
- Good correlation between symptoms, physical examination, and imaging studies.
Not all patients are candidates. Some very large, calcified, or highly migrated herniations, herniations associated with spinal instability, or cases accompanied by severe narrowing of the lumbar canal may require another type of surgery.
When may medical evaluation be urgent?
The patient should seek urgent medical attention if they experience:
- Loss of bladder control.
- Loss of bowel control.
- Numbness in the genital area or around the anus.
- Progressive weakness in one or both legs.
- Disabling pain that prevents walking.
- Fever accompanied by severe back pain.
- Pain after a fall or significant trauma.
These symptoms may indicate serious nerve compression and require immediate medical attention.
Surgical risks
Although endoscopic surgery is minimally invasive, it is still a surgical procedure and may carry risks. The main risks are:
- Bleeding.
- Infection.
- Injury to a nerve root.
- Leakage of the fluid surrounding the nerves due to accidental opening of the membrane that covers them.
- Persistent pain.
- Residual numbness.
- Persistent weakness if the nerve already had significant damage.
- Recurrence of the disc herniation.
- Need for a new surgery.
- Risks related to anesthesia.
The risk of complications is usually low in experienced hands, but it is never zero. That is why it is important to explain the benefits, risks, and realistic expectations to the patient before surgery.
Can the herniation come back?
Yes. Even if the herniated fragment is removed, the disc already has a weakened area. For this reason, there is a possibility that a new herniation may appear at the same level.
To reduce this risk, it is important to follow the postoperative instructions, avoid lifting weight too early, maintain a healthy weight, strengthen the abdomen and gluteal muscles, avoid smoking, and complete proper rehabilitation.
Recovery after surgery
Recovery depends on each patient. In general, pain that travels down the leg usually improves before numbness or weakness. This happens because the nerve may take weeks or months to reduce inflammation and recover.
During the first weeks, it is recommended to:
- Walk progressively.
- Avoid lifting weight.
- Avoid repeated bending.
- Avoid sudden twisting movements of the back.
- Avoid intense exercise until receiving medical authorization.
- Care for the surgical wound.
- Take the prescribed medications.
- Attend follow-up appointments.
Physical therapy may be useful to recover mobility, strength, posture, and confidence when walking. The goal is to return to daily activities safely and progressively.
Warning signs after surgery
After the procedure, the patient should contact their doctor if they experience:
- Fever.
- Drainage from the wound.
- Significant redness around the incision.
- Pain that progressively worsens.
- New weakness in the leg.
- Loss of bladder or bowel control.
- Severe headache when sitting or standing.
- Significant swelling in the calf.
- Shortness of breath or chest pain.
Frequently asked questions
Does endoscopic surgery remove the entire disc?
No. The goal is to remove the fragment of disc that is compressing the nerve.
Does surgery eliminate back pain?
It may improve part of the lower back pain, but its main benefit is usually improving the pain that travels down the leg. If the patient only has lower back pain without clear nerve compression, surgery may not be the best option.
When does the pain improve?
Many patients feel improvement in leg pain during the first few days. Numbness and weakness may take longer to improve.
Can I walk after surgery?
In most cases, yes. Walking is usually an important part of recovery, always following the surgeon’s instructions.
When can I return to work?
It depends on the type of work. An office job may require less recovery time than a physically demanding job that involves lifting weight, bending over, or standing for long periods.
Is endoscopic surgery better than traditional surgery?
Not always. It is an excellent technique in carefully selected patients, but not all cases are the same. Some patients may benefit more from endoscopic surgery, while others may need a different technique.
Final message for the patient
Endoscopic spine surgery is a modern, minimally invasive alternative for treating lumbar disc herniations that compress a nerve and cause sciatica-type pain. Its goal is to release the nerve through a small incision, with less muscle damage and potentially faster recovery.
However, not all herniations require surgery and not all patients are candidates for endoscopy. The decision should be made after a complete medical evaluation, reviewing the symptoms, neurological examination, and imaging studies.
The best result is achieved when there is an appropriate indication, a precise surgical technique, and well-guided rehabilitation.